|
"It's
not my Curve!"
Researcher pioneer
Jellinek coined the expression "the disease concept
of alcoholism" and significantly accelerated the movement
towards the medicalization of drunkenness and alcohol habituation.
In his 1960 book, The
Disease Concept of Alcoholism, Hillhouse, (New Haven), he
identified five different types of alcoholism, and defined
them in terms of their abnormal physiological processes.
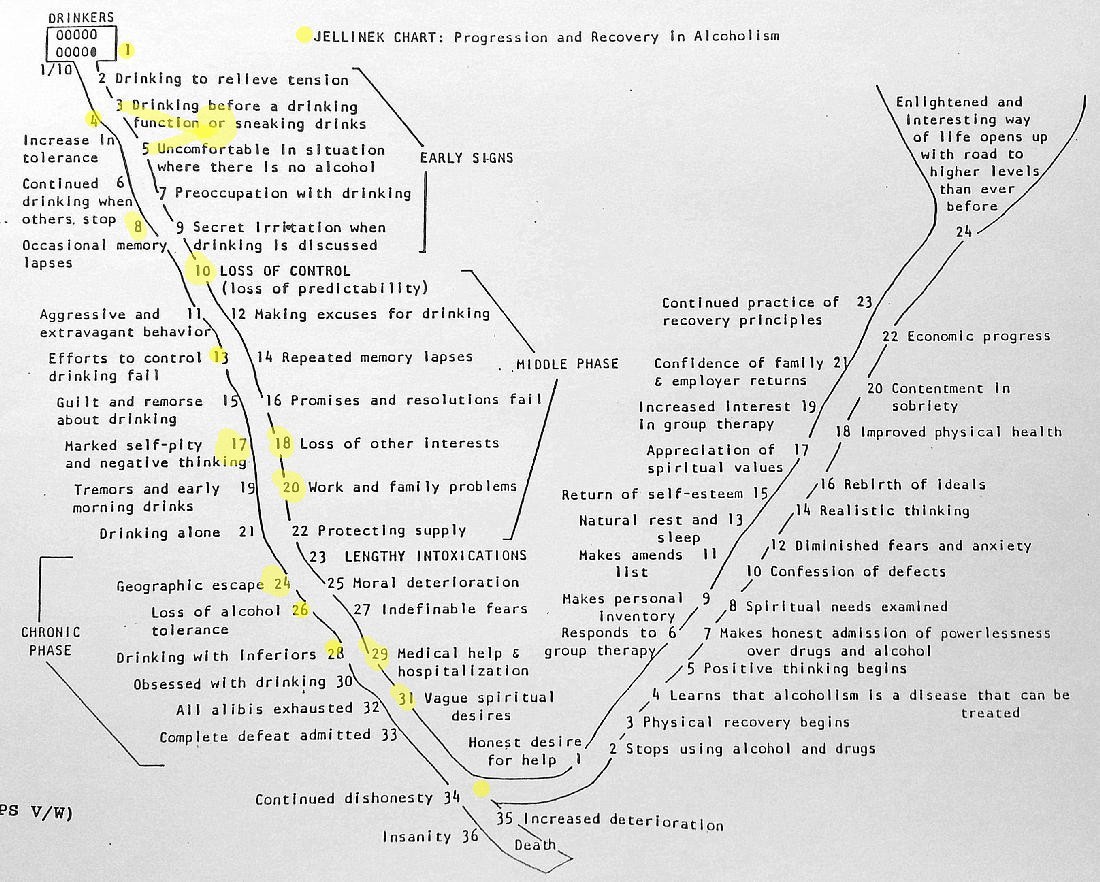
The
"Jellinek Curve" is derived from this classification
of Jellinek, and it was named out of respect for Jellinek’s
work. Jellinek later completely dissociated himself from
this chart's representations; however it is still known
as the "Jellinek Curve".
Read
more about Jellinek .
Talking
Points
Sandy B.: J-Curve
his story
Download
copy of J-Curve
|
Click
on yellow dots for more information.
|
Talking Points.
- Historically: Jellinek
was a pioneer for the disease concept and seeing addiction
on a continuum.
- TASC client is a only
a 3 month blip on their/your screen of life.
- J-Curve provides a
big picture, personal visualization of their addiction.
- Disclaimer: there
is no "one way", Curve is a guide, which supports
the idea there is no one size fits all treatment model.
- Client awareness of
the Curve is just as important as the health care provider's
awareness.
- J-Curve is the form,
client’s fill in their own personal stories, examples.
- Disclaimer: a person
can get off either side at any point, at any time, but
where one lands is unpredictable & it’s getting
back on which can prove difficult.
- Curve accentuates
the concept of time in addiction.
- Metaphors: chutes,
sliding down slippery slope, a ladder, climbing the sequential
steps.
- Client activity: present
the J-Curve as a clinical activity, client circling symptoms
they have experienced.
Going
Down
- The odds: there are
many more people on the DOWN side vs. the UP side.
- The Beginning Box:
10% are “addicted”. But take this into consideration:
take all the people in the US who drink/drug, then whittle
this down by those who abuse their usage, more whittling
to those who get help for their usage, i.e. treatment,
all those, 50% “success”, which leads to the
hard question, what is success? 3 months of sobriety?
1 year? 5? Is abstinence success? Or not having any new
related usage problems? How is this determined?
- Disclaimer: a person
can die from one's first usage, or have a life changing
experience, i.e. killing your friend who's in your car
when you’re driving under the influence, date rape,
alcohol poisoning, etc.
The "Bottom"
- No one can define
another person's "Bottom".
- A “Bottom”
which will motivates a user to make a change, has to be
user driven. All users have a line drawn in the sand,
doesn’t mean they are conscious of that line, though.
- User does not have
to go to the end of the DOWN side to get to the UP side.
- The intersection
between the DOWN and UP, how does one define this area?
Living in hell? “Living but wishing I was dead.”
- Suicide Alert: thoughts,
attempts, actual. Potential is always there, but a “Bottom”
increases the odds.
- There is another
option at the Bottom besides going UP, continuing downwards:
The “Tail”.
- The Big Question:
Why do some people start the UP side while others
don’t?
“Miracle”? Bill Wilson’s “White
Light”? Luck?
Going Up
- UP side is the
least known, misunderstood side.
- Recovery is
more than a matter of just not drinking and/or using drugs,
a family, public perception problem.
- The odds: UP
side is very challenging with the statistics against the
user.
- Relapse Disclaimer:
if one “relapses” (slips) off the Up side,
it's reported they don't get to start at the beginning
of the Down side,
instead they pick up where they left off, immediately,
or in a very short time.
- Disease of Relapse:
yes, people relapse, but do they have to and is the danger
element of relapsing ever emphasized enough for the client?
- Recovery Alert: semantic
vs. active recovery. “Talking the Talking, rather
than Walking the Walk.”
Top
|
Sandy B: J-Curve his story.
One
of the best ways to learn about addiction is to listen
with awareness to recovering people’s stories.
If you aren’t
recovering yourself, attend open AA speaker meetings.
And/or you can listen to AA speaker tapes on YouTube.
A Suggestion:
listen to an AA speaker following along looking at
the J-Curve. Can you identify some of the items on
the Curve in their stories? When did they hit their
“bottom”? And most importantly, what was
it for that individual that turned on the “white
light” allowing them to live in recovery?
Here's Sandy
B's story.
|
Listen
to other AA stories
|
|
|
|